CLINICAL CASE PRESENTATION
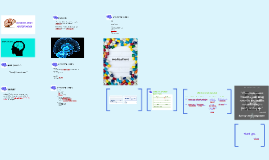
Transcript: PLAN/GOALS OF TX Fix cause IMMEDIATE TRANSFER TO ST VINCENTS + Large parietal/occipital extradural bleed with midline shift +Midline shift >1cm and brainstem distortion on CTB are findings that require rapid and aggressive treatment Whats wrong with this picture??? PSYCHOSOCIAL/ FAMILY: PATHOPHYSIOLOGY of EXTRADURAL BLEED Assessment- interprate this ECG Cameron, P,. Jelinek, G., Kelly, A., Murray, L. & Brown A,F, T. (2009) Textbook of Adult Emergency Medicine 3rd edition. Sydney: Churchill Livingstone Elsevier Chauvet, D., Reina, V., Clarencon, F., Bitar, A. & Cornu, P. (2013) Conservative Management of Large Occipital Extradural Haematoma. British Jounral of Neurosurgery, 27 (4), 526-528. Nadig, A, S. & King, A. T. (2012) Traumatic extradural haematoma revealed after collateral decompressive craniectomy. British Journal of Neurosurgery, 26(6), 877-879. Urden, L, D., Stacy, K, M. & Lough, M. E. (2014) Critical Care Nursing: Diagnosis and Management. St Louis, Missouri: Elsevier CTB results...... MORPHINE - sedation/analgesia Clinical Case Presentation - Ms Jones Traumatic Brain Injury MIDAZOLAM - sedation MANNITOL ACTION: GABA receptor agonist, chloride channel activation Advantages:- rapid onset/offset, reduces ICP, raises seizure threshold, less hypotensive than propofol +highly lipid soluable, + metabolised by liver Disadvantages:- can reduce MAP, delirium, withdrawl syndrome, resp & cough supression Dosage: induction 0.1/kg Maintenance sedation 0.01-0.2/kg/hr Pharmcokinetics : onset 6min, hepatically metabolised, Advantages: long term analgesic, hyponotic agent, low cost, haemodynamic stability Disadvantages: hypotension, bradycardias,respiratory & cough depression, constipation, nausea, Doseage : 0.05-0.1mg/kg Given as infusion Morph50mg/Midaz 50mg in 50ml Action: osmotic diuretic, elevates blood plasma osmolarity, thereby enhacing excretion of water from tissues as a result cerebral odema, elevated ICP is reduced Advantages:Reduces acutely raised ICP and cerebral oedema in critical care. Disadvantages:- fluid overload, rebound cerebral oedema Dosage: 0.05-0.1/kg PATHOPHYSIOLOGY of EXTRADURAL BLEED Sinus bradycardia 42 BPM flatterned T waves in LI,II &III & V5 &V6 +Maintenance of airway +Maintenance of cerebral pressures +Correct hypotension (systolic >90mmHg ) & hypoxia (PaoO2 > 60mmHg ) + sedation & analgesia - Morph/midaz + 30 degrees head up to < ICP +immediate transfer to St Vincents Hospital for Neurosurgery Patient Presentation Intubation Stabilise patient :- stabilise airway NPA, prepare for intubation. RSI- Fluid preload, Prop 40mg , Midaz 5mg and Suxamethonium 100mg IV to sedate and intubate. Adequate sedation and analgesia infusion-Morph/midaz CTB Maintain pt at 30 degree angle Maintain O2 and perfusion for cerebral blood flow NGT CXR Nursing and medical mangement TIME IS BRAIN Intubated size 7.5 ETT 22cm at lips SIMV volume control Vt 500, RR 2o, Fio2 100% Peep 5cm H2o, ETCo2 42 on monitor Morphine/Midaz infusion commenced Propofol boluses for aggitation Taken to CTB + Serous & uncommon complication of head injury + Occurs in only 3% of TBI, 75% in skull fractures + Injury to blood vessel causing formation of haematoma by stripping the dura mater from the skull +It is important to remember to involve the family, communicate honestly and effectively +Ensure adequate supports in place. + Involve care-co +If care-co not avail provide couseling to immediate family when appropriate +46 YO Female was BIBA after witnessed fall at a wedding. +Headstrike & lac to occiput +Nil LOC or seizure activity. +6-7 ETOH drinks on board + Recently fit and well +Past medical hx - C section +Medications- NIL +NKDA + 200mg IN Fentanyl, 10mg IV Maxalon on route via IVC R) hand Setting the scene + Maintenance of adequate tissue metabolism via ensuring delivery of oxygen, fuels to meet cellular demand. Cerebral perfusion pressure (CPP) Mean arterial pressure (MAP) Intracranial pressure (ICP) Cerebral Blood Flow MAP-ICP= CPP PRIMARY SURVEY A- Obstructed, requiring jaw thrust & suction of vomit, NPA insitu B- Spont resps requiring BVM, laboured breathing, Sp02 ?94% C- PW slight diaphretic, HR 40-70 SB-SR with pauses, bilat IVC, stat fluids, manual BP 150 systole D- uneven pupils, GCS4, decerebrate posturing E- C spine precautions, lac to occiput ASSESSMENT Stages of compensation & decompensation in intracranial hypertension Cushing's reflex/ triad +The presence of HTN, bradycardia and abnormal respirations associated with increased intracranial pressure (ICP) +Late finding +Sympathetic nervous system is activated = peripheral vasoconstriction, inc in cardiac output to inc MAP MAP> ICP = restored blood flow +Baroreceptors in carotid bodies detect high pressures and respond by dramatically reducing HR. Setting the scene + Initally GCS 14-15 E3V5M6 + Haemodynamically stable + During AV handover pt rapidly deteriorates GCS 4 E1V1M2 + Irregular pupils + Airway obstruction + Immediate transfer to Resus + Prepare for